A man in his early 30s touches his feet for the first time in years.
A teenage girl, with pretty intense toe-walking, was having trouble getting up and down stairs.
A martial artist in her 50s leveled her “anterior pelvic tilt” after 20 years—just by getting her heels on the ground.
A woman in her 60s had a duck walk, and one of her heels just couldn’t touch the ground. She cried when she felt the floor under her feet for the first time in ages.
Posture starts with the feet. It doesn't matter if the issue is head forward posture, a hunched back, a curved spine, or a tilted hip—it starts with the lower extremity, and quite often, at the foot itself.
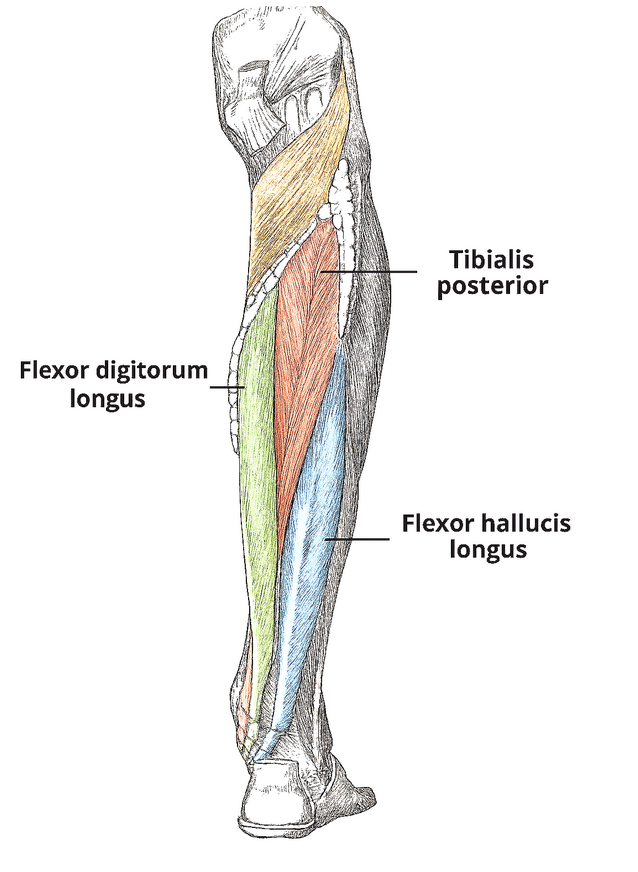
Think of muscles like pistons. They are designed to move independently up and down in their tubes (fascial sleeves). However, over time, they get sort of glued together—or gummed up. In the case of the foot, there is a group of muscles in the lower leg we call Tom, Dick, and Harry (Tibialis Posterior, Flexor Digitorum Longus, and Flexor Hallucis Longus). They live in the deep posterior compartment of the calf—tucked away underneath the more prominent calf muscles.
Over years of abuse (life in the modern world—sedentary lifestyle, wearing bad shoes, walking on hard surfaces), they begin to stick to the muscles on top of them (the superficial ones). When this happens, both layers are restricted. They have to negotiate movement together.
It’s sort of like hanging out with a group of friends, but each of you is trying to go about the day as you would solo—and everyone has different ways of doing things. It just doesn’t work.
Sam (Soleus) agrees that she definitely wants to grab that mocha in a bit… but she keeps leading you to shop after shop, stop after stop. The group is moving slowly—nowhere—when the coffeehouse is right there. It’s right there, Sam! Then there’s the rest of the pack, who can’t make a decision to save their lives. Maybe they just don’t want to offend anyone, by communicating their actual wants or needs, so they leave the decision up to the group. You know… an informal democracy that doesn’t really get anything done.
And you, you’re Tom, in this analogy by the way, and all you wanted was to get your mocha… you’re fine loitering, lollygagging, or even moving at a snail’s pace… your also okay with plodding, creeping about, and lurking. You’d be perfectly content dragging feet, hobbling, and limping along. To be absolutely clear, you, my friend, you are completely fine taking yours and everyone else’s sweet time – as long as you can at least start your freakin’ journey, like a normal freakin’ human being (or muscle) with some freakin’ caffeine!
But no. This group of indecisive people (glued-together muscles) can’t seem to move in any orderly fashion. They just sort of meander, directionless, as a pack—like that entire family of six who decided to shop together, on a flippin’ Sunday, in the tiny aisles of Trader Joe’s last week. You know who you are!
Now where was I? Oh yes, “Tom” was trying to get a mocha (pull up on the arch), but Tom and Dick are glued (have formed adhesions) to Sam. Tom made the mistake of carpooling… he will not make that mistake again. Sam is currently deep in conversation with Nicole (adhered to Gastrocnemius), preventing Tom from getting his caffeine fix. And Nicole is way more interested in window shopping (flexing the knee joint) at the moment—and oblivious to the effect she’s having on the group dynamic (pulling up on the heel, preventing it from touching the ground). So Gastrocnemius is pulling up on the heel, and Soleus too, by default. At the same time, Tom and Harry are trying to get a mocha (pull up on the arch).
Meanwhile, Tabitha, Tom’s sister (Tibialis Anterior), is working on her master’s thesis while sucking down a tremendous amount of espresso at the very coffee shop he’s been trying to get to all morning (also pulling up on the arch—but from the opposite side). Without her brother there, she might consume too much coffee and get super cracked out (lift up on the outer arch further collapsing the inner). Tom should have taken his sister’s offer and studied together… why Tom, why?!
Meanwhile, Dick is also just trying to get to the record store (which Sam also promised to go to) for The Phalanges EP: Gripping the Floor with Our Toes. His plan all along was to grab a cold brew and then hit the record store.
What’s up with Harry in all of this? While he’s certainly interested in checking out the new record, he’s mostly along for the journey—the group hang—to provide some structure to the whole endeavor (big toe push-off and propulsion).
By the time 3:00 rolls around, the group has somehow found their way to an ice cream shop. No coffee. And now it’s too late for reasonable people to caffeinate. The entire group is tired from all the push-me-pull-you of the endeavor. They cave. They overindulge. [The end.]
What I’ve just described is a very common phenomenon: Muscles, ligaments, and the tiny bones of the ankle and foot—each designed for highly specialized, dynamic functions—become bound together by fuzzy scar tissue.
The lower leg and foot are completely exhausted when this dynamic occurs. Muscles end up performing tasks they aren’t meant to—some in an effort to support those that can’t function properly, others simply because they’re stuck going along for the ride.